
Parts 1 and 2 of this series discussed the anatomical structure of the core and the correct method of core activation. Establishing efficient stabilization of the spine and pelvis is essential to injury prevention not only in sport but in the activities of daily living as well. The following is a review of what has been covered so far.
- The core is made up the the diaphragm, the muscles and fascia of the abdominal wall, the thoraco-lumbar fascia, the muscles of the pelvic floor and the lumbar multifidus.
- Each component of the core has specific function.
- Strategies that isolate one portion of the core are ineffective and create dysfunctional patterns.
- The individual parts of the core are designed to work together as a functional unit for the purpose of generating and regulating intra-abdominal pressure.
- Spine and pelvic stability starts with intra-abdominal pressure.
- There are two predominant theories of core activation.
- One method of core activation is abdominal hollowing or pulling the navel toward the spine. This approach isolates the transversus abdominis and has been found to be an ineffective method of stabilizing the spine.
- A second strategy uses an abdominal brace. Research has found that bracing to be a far more effective than hollowing but care must be taken to not over-brace.
- Lastly, the core’s ability to effectively generate IAP and create efficient stability depends on maintaining ideal neutral posture.
Effective Stabilization
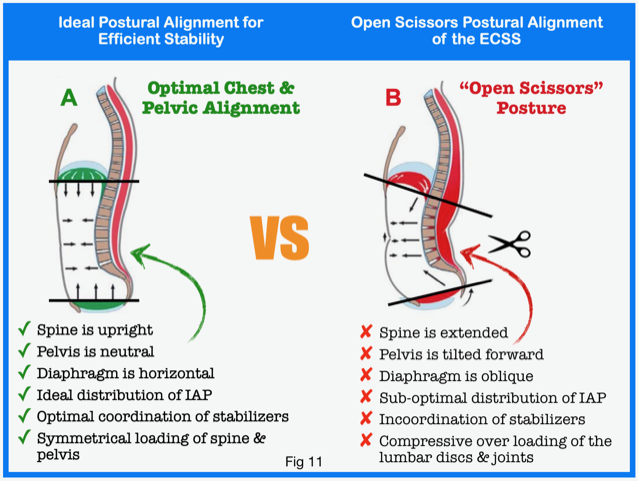
Effective core stabilization is crucial for injury prevention not only for athletes but for the non-athlete performing the normal activities of daily living too. As the title of this series suggests, stability must come from the inside-out. That is, stability begins on the inside by generating intra-abdominal pressure. The ability of the core to generate optimal intra-abdominal pressure (IAP) requires the maintenance of ideal postural alignment. The image below in figure 11 depicts the ideal postural alignment of the diaphragm in relation to the pelvic floor for generating and maintaining efficient stabilization of the spine and pelvis.
To maximize IAP, the diaphragm must be positioned parallel to and directly over top of the pelvic floor. With ideal posture, IAP can be distributed multi-directionally. The force of IAP pushes backward against the spine. IAP is also directed outwards into the abdominal wall causing it to stretch. Loading the abdominal wall will in turn load the thoraco-lumbar fascia. The net effect of these forces is designed to balance each other thus creating a buttress that holds this spine in place. This strategy prevents isolated compressive loading of individual segments in the lumbar spine. This is an “inside-out” strategy and the basis for both static and dynamic stability. What if an “outside-in” strategy were used instead? What would be the impact on stability if someone did not have a physiologically normal respiratory pattern?
Extension/Compression Stabilization Strategy (ECSS)
We will now turn to a compensatory stabilization strategy that is very common in both athletic and non-athletic populations. The Extension/Compression Stabilization Strategy or ECSS is a pattern of compensatory stabilization that utilizes an “outside-in” approach. That is, this is a strategy that is focussed on activating structures that are outside of the core rather than initiating stabilization with intra-abdominal pressure. As outlined earlier, “outside-in” approaches are not natural, efficient or effective.
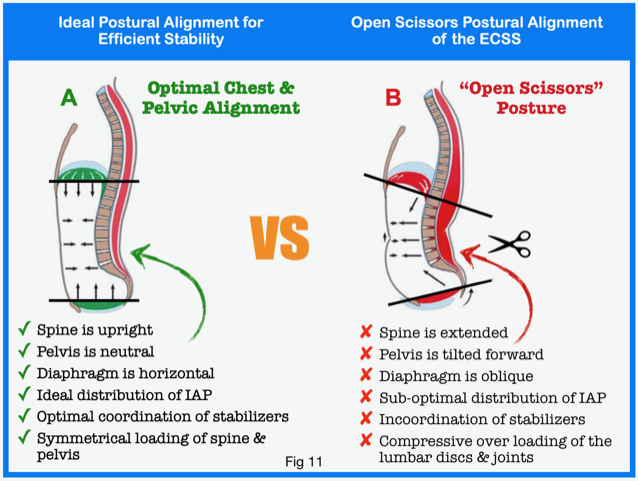
The ECSS method of lumbopelvic stability is perhaps the most common underlying cause of lower back pain as well as a myriad of other mechanic pain syndromes that plague modern civilization. As the name of this strategy suggests, it involves an extension posture and chronic compressive loading by hyperactive spinal erectors to achieve stabilization. There are three key mechanical consequences to extension of the lumbar spine. First, because the spinal joints sit at the posterior side of the spine, an extension posture whereby the curvature of the lower back is increased, causes the joint spaces to close down and the joint surfaces pinch.
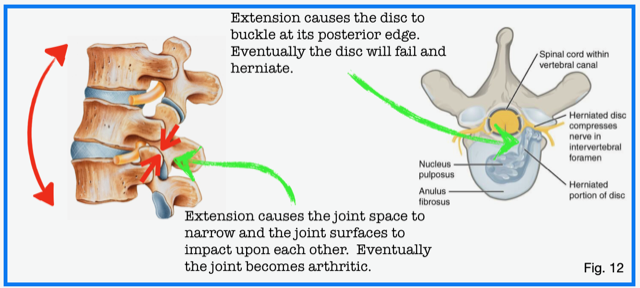
Secondly, as the spine moves into extension the posterior edge of the disc will buckle and bulge. Chronic postural loading in extension causes the joint surfaces to break down and become arthritic. The disc too will fail over time. The physical stress of loading in an extension posture causes the wall of the disc to develop micro-fissures. With time these small cracks will coalesce to form a large tear that extends through the full thickness of the disc wall. Eventually the disc bulges and herniates. These two problems of joint impaction and disc loading are compounded by the over-activation of the lumbar erectors that further enhances compression of the joints and discs. Lastly, having a lumbar extension posture will directly impact the ability to generate and distribute IAP. As noted above, optimal generation and distribution is the basis of static and dynamic stabilization. This can only occur when the diaphragm and pelvic floor are positioned parallel to each other. The “Open Scissors” posture that characterizes the ECSS places the diaphragm and pelvic floor oblique to each other. As a result, the amount of IAP generated is compromised. The distribution of IAP is also effected. The hallmark physical signs of this compensatory strategy are readily identifiable.
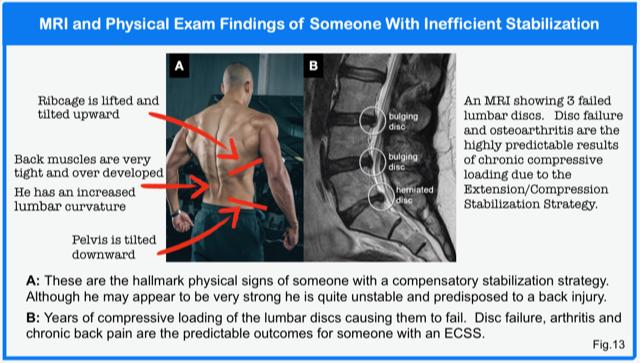
The image above in figure 13 depicts the “Open Scissors” postural distortion that typifies the ECSS. The chest is lifted and the ribcage is flared in a person who uses the ECSS. Their pelvis is typically rotated downwards. With this postural distortion, the diaphragm and pelvic floor are not in parallel but are oblique to each other. A person with this pattern will naturally not be able to generate intra-abdominal pressure very effectively. Nor will they be able to distribute that IAP in way that will allow for efficient spinal stabilization. Instead, they will fruitlessly rely on ever more spinal extension and compression to meet the demand for ever more stability as their activity dictates. Consequently, the lumbar and lower thoracic paraspinal muscles are particularly tight and often over developed.
Muscles can be classified based upon their function as a stabilizer or a mover. Muscles that function to provide joint stability are small, positioned close to joints and are very richly supplied with nerve fibers. These characteristics provide an ideal environment for muscles like the multifidus, rotatores and longus colli/capitus to provide joint stability and motor control. Conversely, large multi-segmental muscles like the spinal erectors, quads, latissimus dorsi, pectorals and upper trapezius function to create movement and power. They are much less densely populated with nerve fibers and are therefore poorly designed to provide joint stability. When someone adopts a compensated stabilization strategy like the ECSS, the larger and more superficial muscle groups compensate for the inherent lack of stability and become dominant over the smaller, deeper muscle groups. In addition to the large muscle groups being poorly designed for motor control and stability, they are also capable of generating much higher levels of compressive loading. The combination of diminished motor control and joint instability along with excessive joint loading predisposes one to trauma and accelerated wear and tear.
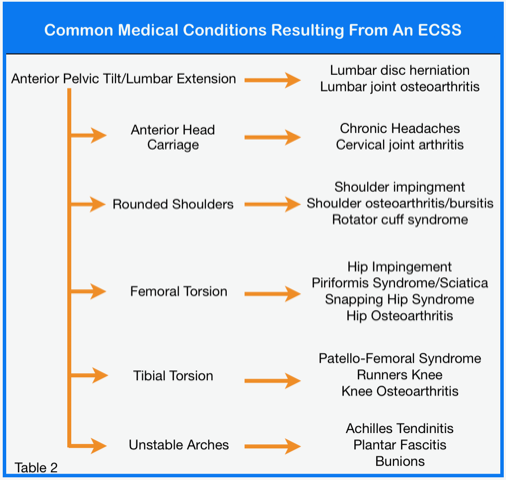
The compensatory changes noted above are not limited to the lower back and pelvis either. Keeping with stereotypical findings of someone with an Extension/Compression Stabilization Strategy or an “Open Scissors” posture are: an anterior head carriage and rounded shoulders; femoral torsion; tibial torsion and dropped arches. Each of these postural changes has their own list of medical sequelae or syndromes. The table above outlines the widespread effects of adopting a suboptimal posture or relying on an Extension/Compression Stabilization Strategy. This mechanism explains why we are plagued with so many physical complaints especially in the absence of any significant trauma. We are often told by healthcare practitioners that injuries of a non-traumatic origin are age related or an overuse syndromes. Neither of these terms could be further from the truth. People do not acquire muscle and joint injuries merely because they are getting older. Nor do injuries occur because people move too much. People become injured because they do not control their movements. Stability begets posture. Posture begets stability. The manner in which we stabilize and the posture we favour dictates the patterns with which we move. There are consequences to inefficiency; if someone does not stabilize with an ideal pattern then a compensatory pattern will dominate. The more we move, exercise or train with a bad pattern the more we reinforce that bad pattern. In other words, if we continue to do what we do we will continue to get what we get. The solution is not about making something stronger, training harder, lifting heavier weights, wearing a brace or using some gadget. The solution, to be discussed in the next part of this series, starts with identifying the origin of the problem and building good patterns.
Key Points
- All compensatory stabilization strategies use an “outside-in” approach to provide stability. They are unnatural, inefficient and ineffective.
- Getting stronger will not fix a compensatory strategy. Exercising with a bad pattern will only reinforce that bad pattern.
- The Extension/Compression Stabilization Strategy is a very common underlying cause of lower back pain and a myriad of conditions that affect the neck, shoulders, hips, knees and feet.
References:
- Shahraki, N M et al Prediction of clinically relevant initiation and progression of tears within the annulus fibrosus. Journal of orthopaedic research. January 2017.
- Sahrmann, S. A. (2000). Diagnosis and Treatment of Movement Impairment Syndromes. Mosby, USA. In Press.
- Kolar, Pavel (2013). Clinical Rehabilitation. ISBN-10: 8090543804. In Press
- Thiem, Trevor et al. Postural Restoration Institute. Retrieved February, 2019. https://www.posturalrestoration.com
- Ulm, Richard. Compensatory Stabilization- The Extension/Compression Stabilizing Strategy. Retrieved February, 2019. https://www.athlete-enhancement.com/articles
About the Author:

Dr. Morris Gasparin is full body level 1 & 2 Active Release Techniques certified. He has been incorporating the DNS method of evaluation and rehabilitation since 2012 and been in private practice at Cloverdale Chiropractic since 1995.