
In the first two parts of this series we discussed the anatomical structure of the core and the correct method of core activation. The mechanics of turning intra-abdominal pressure into pelvic and spinal stabilization was also reviewed. Establishing efficient stabilization of the spine and pelvis is essential to injury prevention not only in sport but in the activities of daily living as well. In part 3, we examined the consequences of adopting a very common but unnatural and inefficient stabilization strategy called the ECSS or Extension Compression Stabilization Strategy.
The following is a review of what has been covered so far.
- The core is made up the the diaphragm, the muscles and fascia of the abdominal wall, the thoraco-lumbar fascia, the muscles of the pelvic floor and the lumbar multifidus. Each component of the core has specific function and are designed to function as a unit to generate and regulate IAP.
- All strategies that isolate one portion of the core are ineffective and create dysfunctional patterns.
- It is from intra-abdominal pressure that spinal stability is made possible.
- There are two predominant theories of core activation. The core’s ability to effectively generate IAP and create efficient stability depends on maintaining ideal neutral posture.
- The Extension/Compression Stabilization Strategy is a very common compensatory pattern. It is an inefficient means of stabilizing and frequently is the underlying cause of several syndromes involving not only the lower back, but the neck, shoulders, hips, knees and feet too.
Our discussion will now turn to a method of evaluating and correcting inefficient stabilization and compensatory movement patterns.
Dynamic Neuromuscular Stabilization (DNS)
Dynamic Neuromuscular Stabilization, or DNS as it is more commonly referred to, was developed by Professor Pavel Kolar, PT, PhD, Director of the Rehabilitation Department, University Hospital Motol School of Medicine, Prague, Czech Republic. Dr. Kolar was profoundly influenced by his instructors Professors Karel Lewit, Vladimir Janda, Vaclav Vojta and Frantisek Vele of the Prague School of Rehabilitation in the Czech Republic. DNS is not a technique. Rather, it is a method of assessment and rehab designed to improve motor control and efficiency of movement. The strategy of DNS is to assess and activate the body’s inborn stabilization mechanisms that are based upon the scientific principles of Developmental Kinesiology. This description is typically how the DNS concept is explained in research circles. What exactly is “Developmental Kinesiology” and how does this relate to core stability and musculoskeletal pain? Most people would be at a loss to explain the meaning of these terms or how they are related to their back or hip pain. It is my experience that most healthcare professionals would also struggle to comprehend this relationship unless they are experienced with the DNS approach.
Developmental Kinesiology (DK)
What is Developmental Kinesiology? Humans, unlike almost every other mammal, are incapable of producing any purposeful movement at birth. Most animals are able to run within a few hours of being born. However, for humans, movement and stabilization have to be developed. The theory behind DK is based upon the development of motor function in early childhood which is genetically pre‐determined and follows a predictable pattern. As the brain and the rest of the central nervous system matures, the baby develops new postures and movement patterns based upon their stage of development. Previously in this article series we discussed how core stabilization is completely predicated upon the diaphragm’s ability to generate intra-abdominal pressure. An infant will never develop efficient stabilization without first having a physiologically normal respiratory pattern. For the first 4½ months the baby is developing adequate core stabilization. It is only when efficient stabilization is developed can the infant begin to produce purposeful movement. Therefore, respiration and IAP precede stabilization and stabilization precedes movement. The quality of stabilization dictates the quality of movement. That is, a baby cannot develop the correct postural position or movement pattern if the requisite stabilization for that movement or posture is not already present.
With the basic core stabilization pattern in place, the infant then develops all the movement patterns necessary to roll over, sit up, crawl and eventually walk. The most fascinating phenomenon in baby development is that all the correct movement patterns are “pre-wired” in the baby’s brain. Neurologically healthy babies do not have to be taught how or when to roll, sit, crawl and walk. Yet they all do it the same way, at roughly the same age, and with perfect stabilization patterns.
There is also a strong correlation between CNS maturation and the structural or anatomical development of bones and joints. As noted above, maturation of the brain influences development of motor patterns. Equally important is the influence of CNS maturation on structural development. This relationship between the CNS, motor programming and skeletal development is very apparent in the presence of a CNS lesion. For example, in children with cerebral palsy, where muscle coordination is adversely affected, there are subsequent marked abnormalities of their hip joints. In short, not only is stabilization necessary for developing normal movement patterns, but it is also required for normal skeletal development too. Therefore, an optimized musculoskeletal system in both the developing infant and adult populations requires good stabilization, and efficient movement patterns. Logic would then lead one to conclude that the DK stabilization strategies and movement patterns would make for an ideal standard for assessing motor control and movement patterns in the adult population. It should also seem reasonable that if a pattern is observed in the adult population that alters from this ideal standard, it should result in a highly predictable outcome of musculoskeletal pain, tissue or joint failure and injury.
Joint centration
As noted above, the basis of the DNS approach to assessment and rehabilitation is founded upon the scientific principles of developmental kinesiology. That is, DNS uses the same postural positions, movement patterns and stabilization strategies that a neurologically healthy infant develops during the first 16 months of life as a gold standard for analysis and rehabilitation for adults. DNS considers these developmental patterns as ideal because neurologically healthy infants have not been negatively affected by cultural influences, trauma, bad habits, poor posture or training errors. They have a physiologically normal respiratory pattern; they use the most efficient stabilization strategy; they move with perfect alignment and they maintain ideal joint centration. Comparing the way in which people function to these gold standards provides considerable clinical information about the origin of their physical complaints and how best to correct them.
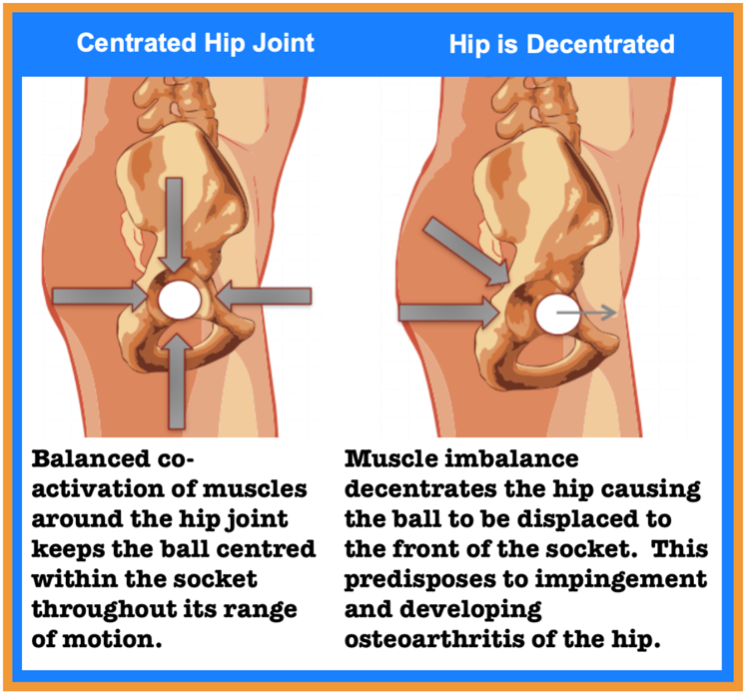
Joint centration refers to the ideal alignment of one bone relative to another. Centration is not just about a joint’s static position. More importantly, joint centration is a dynamic concept that refers to the ability to maintain that ideal joint alignment throughout a range of motion. This optimal positioning of two bones relative to each other allows for maximal load transfer across the joint with minimal risk of injury. When joints are properly centrated, movement occurs in the most economical fashion and muscles can generate power to their full potential.
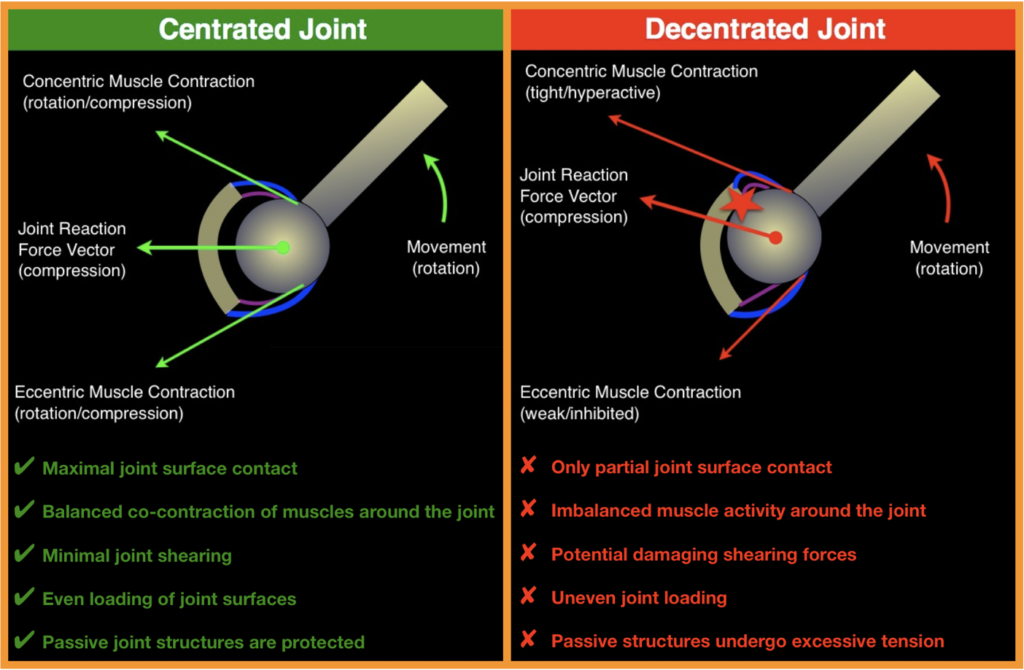
The opposite of centration is called joint decentration. Decentration is the definition of an unstable joint. Any joint that is decentrated is poorly positioned to bear weight or allow for smooth and efficient movement. Take for example the hip joint. All the forces that act upon the hip have to be balanced. The head of the femur cannot be held centred in the hip socket throughout its entire range of motion if there is a muscle imbalance acting upon it. Most often we see people gripping with their glutes in an attempt to support themselves. This will cause the ball of the hip to become decentrated to the front of the socket. The loss of centration causes hip impingement. Over time the joint surface begins to breakdown and becomes arthritic. Ligaments, joint capsules, tendons, muscles and cartilage; all the structures in close proximity to the decentrated joint are affected by compensatory overload. All of the tissues at the hip are predisposed to injury.
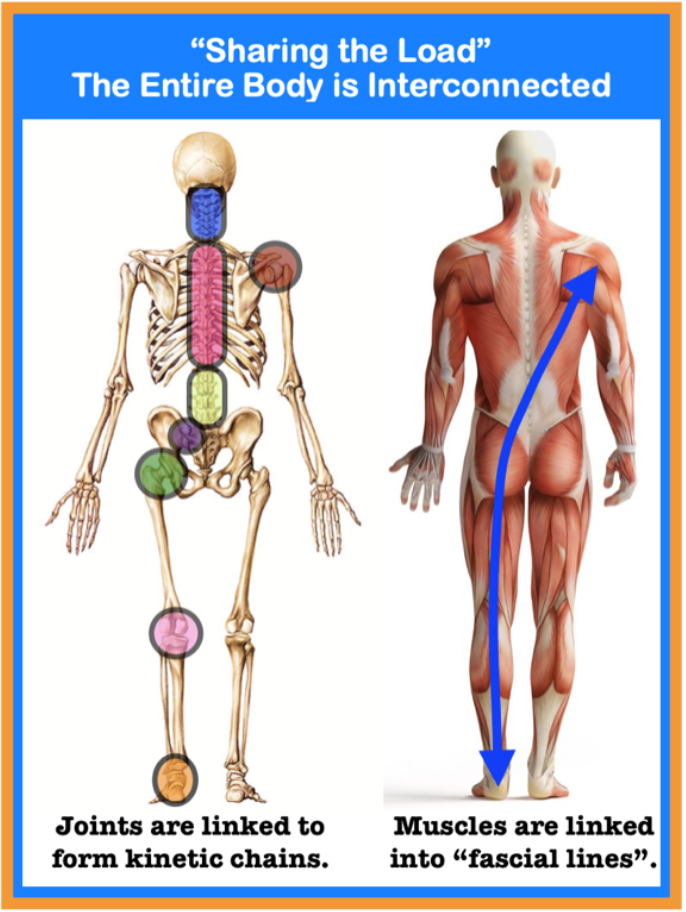
The negative effects of joint decentration are not localized to only that particular joint either. The entire kinetic chain is affected too. A kinetic chain, or kinematic chain as it is sometimes referred to, is the concept of linking muscles and joints in a chain whereby movement of one segment affects the entire chain. The kinetic chain concept also helps predict how forces are created, transmitted and absorbed along a chain. The kinetic chain, from the foot to cervical spine, has to compensate for the lack of hip centration. Therefore, injuries can occur anywhere up or down the chain because of a hip problem. The opposite is also true. Perfect stabilization and ideal movement patterns require perfect joint centration throughout the entire kinetic chain. A disturbance anywhere in the kinetic chain can cause the hip to decentrate. Inefficient stabilization strategies, such as the ECSS; sucking in the abdominals; bad postural habits and injuries predispose one to joint decentration. Most often the origin of a problem is not where the pain is. For example, someone may have a shoulder complaint, but the actual underlying cause probably started somewhere else. Take for example baseball pitching legend Dizzy Dean. Jay Hanna “Dizzy” Dean was a right-handed pitcher for the St. Louis Cardinals. To call him an elite athlete would be an understatement. In his career he complied 1,163 strikeouts; twice he was the MLB wins leader and four straight years the strikeout leader. He was also the last pitcher to record 30 wins in one season. During the 1937 Allstar game he took a line drive hit off his left big toe causing it to fracture. With the season on the line, he was pressured to return to playing before his toe was completely healed. He noted that because he could not plant his left foot correctly, he had to change his throwing motion and could not position his right shoulder to throw the ball. His throwing mechanics changed starting at his foot. The shoulder could not handle the stress and eventually he was injured. 37 games after that injury to his foot, Jay Hanna “Dizzy” Dean had to retire from major league baseball. This is a perfect example of the importance of maintaining the integrity of the entire kinetic chain.
Two things should be immediately clear. First, optimal stabilization encompasses the entire kinetic chain. Let’s stay with the shoulder joint as an example. The rotator cuff muscles stabilize the shoulder joint. Their ability to function is directly dependent upon how well someone can position their shoulder blade. If the shoulder blade is winging or is in an incorrect postural position, the rotator cuff will have to work too hard. It is impossible to position the shoulder blade and control its movements correctly if the head or ribcage are stabilized in a less than ideal position. It is impossible to position the head and ribcage correctly if the arch of the foot collapses or the hip drops when weight bearing on that side. Each link in a kinetic chain is dependent upon the rest of the chain. When centration is lost anywhere in the chain, the entire chain is compromised and the weakest link will fail – it is only a matter of time. A second important point is that posture, movement patterns and motor control are all dependent on having a physiological normal respiratory pattern which must be maintained while moving.
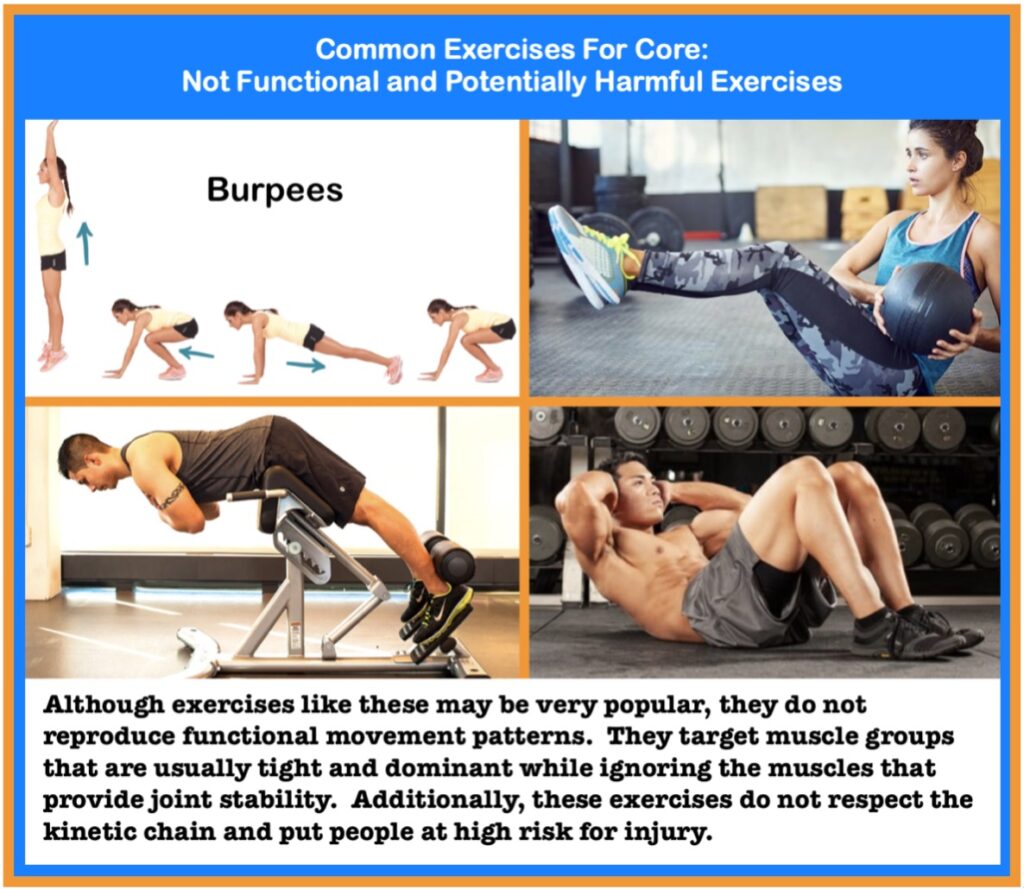
Therefore, corrective exercise programs must incorporate the entire kinetic chain. It is not enough to simply train a muscle in isolation. Traditional rehab exercises for the shoulder that focus on isolation training have poor clinical outcomes. Since the shoulder, or any other body part for that matter, does not function in isolation from the rest of the body, why would anyone train it that way!
So, what does the DNS approach have to do with kinetic chains and joint centration? How does DNS differ from any other strategy for improving strength, coordination, mobility and stability? What sets DNS apart begins with the assessment. As noted previously, the assessments and corrective exercises used by DNS practitioners are based upon the stabilization and movement strategies of neurologically healthy infants. By carefully comparing the clinical population to this “gold-standard”, the DNS practitioner is able to identify where in the kinetic chain that the system failed.
DNS Assessment and Correction
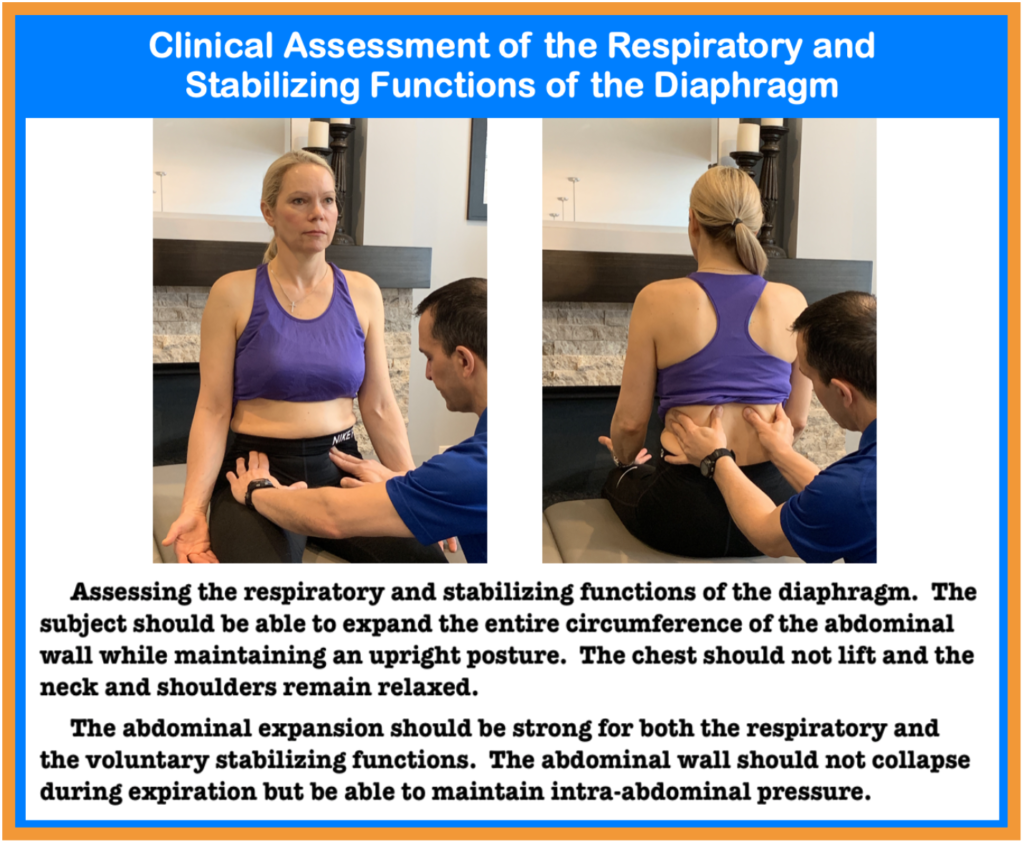
The clinical assessment begins with testing the respiratory and stabilizing functions of the diaphragm. This article series has consistently stated two things. First, stability begins with respiration. Second, the primary function of the core is to generate intra-abdominal pressure. It makes logical sense then that respiration and the ability to generate IAP would be the logical place to start if we are assessing the quality of a person’s stability and movement patterns. In the words of Karel Lewit, paediatric neurologist and the world authority on musculoskeletal medicine:
The DNS practitioner then compares a patient’s posture and movement patterns to the developmental positions of healthy infants. This comparison helps identify where in the kinetic chain the system failed. In the case of an old injury, compensatory movement patterns are sure to have developed. Abnormal movement patterns and painful trigger points are a protective mechanism against further injury. Unfortunately if bad motor patterns are allowed to continue, unstable joints and strained tissues wear down. Over time this may lead to chronic pain and degenerative conditions, such as arthritis, tendinitis, bursitis, disc bulging, herniation and degeneration.
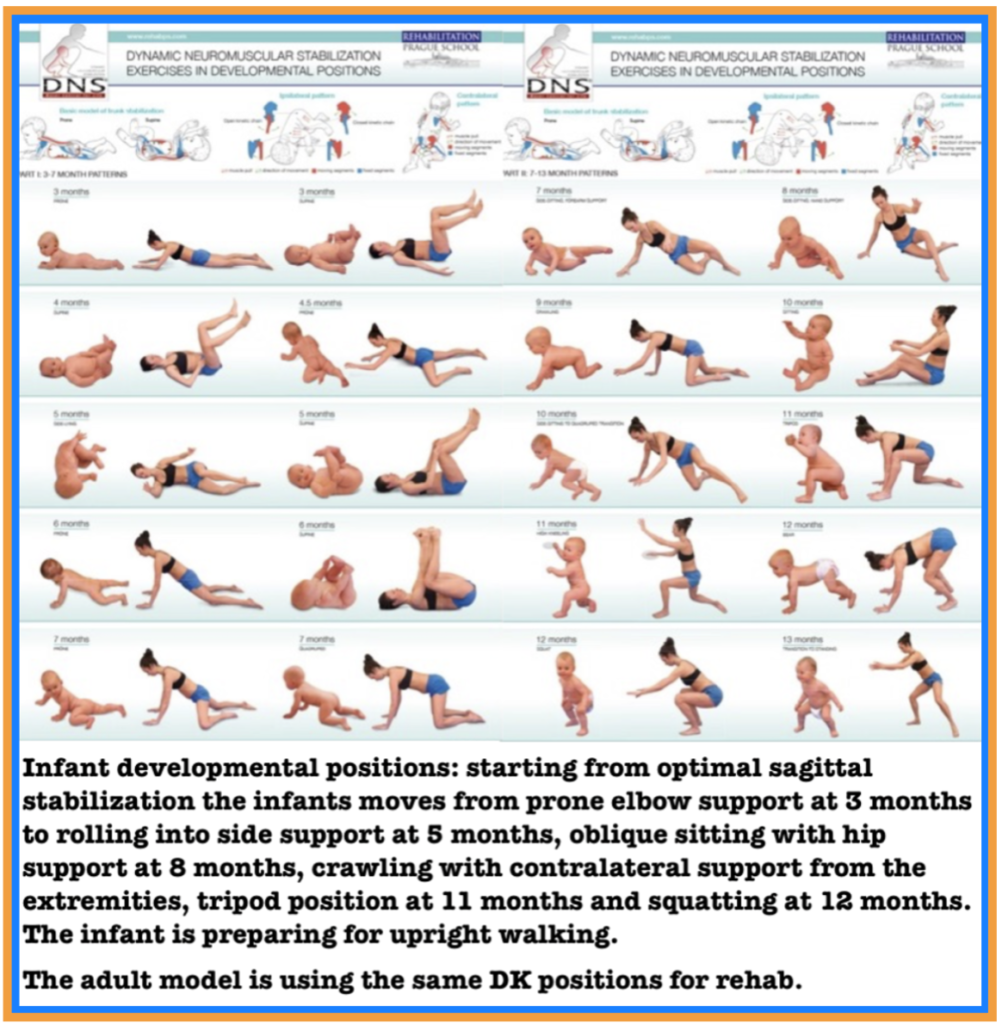
The image above shows the developmental positions that infants transition through as they mature. These DK positions, as previously discussed, promote joint centration throughout the entire kinetic chain. To perform them correctly requires the balanced co-activation of muscles. The progression from back lying, to side lying, to knee support, to elbow support etc requires global muscular interactions that allow us to become upright in the vertical plane during the first year of life. Understanding these global muscle interactions, identifying their deficits, and how to restore muscular synergy for ideal movement is the goal of DNS. Amazingly, adults can use these same developmental positions to retrain efficient stabilization and movement patterns.
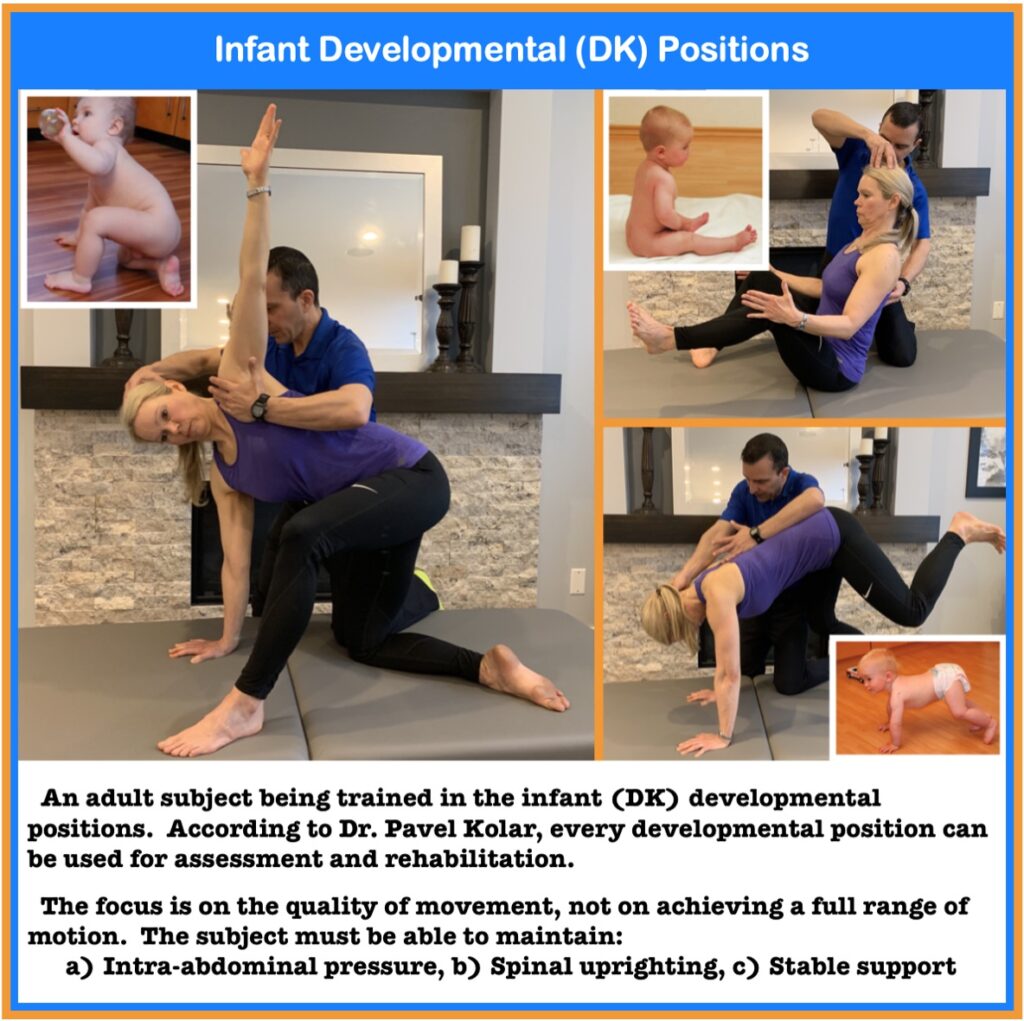
The original programming that was present in the developing infant is still present in the adult. The programming just needs to be “found”. According to Dr. Kolar, “every developmental position can be used as an exercise position.” The developmental positions that DNS uses can be modified into functional exercises that help us to “find” the proper motor program that has been “misfiled”. However, each exercise must follow the same basic principles:
- Restore proper respiratory pattern and IAP regulation through breathing exercises
- Establish a good quality of support for any dynamic movement of the extremities
- Ensure that all joints are well centred throughout the movement
- Resistance or load should match the person’s ability to maintain proper form during the exercise or drills
The support function of muscles around a joint are most often what has become dysfunctional. It is important to realize that it usually is not the lack of muscle strength but the inability to activate the muscle properly that is the problem.
To restore the normal pattern we have to perform exercises which challenge that specific support. The ultimate strategy is to “train the brain” to maintain central control, joint stability, and ideal quality of movement that is achieved through guidance from the clinician. Eventually, through repetition of the exercises, the central control establishes an automatic model that becomes a fundamental part of everyday movement and skills.
Integration of an ideal pattern of stabilization in sport or the activities of daily living will not only reduce the risk of injuries and secondary pain syndromes resulting from overloading, but may also improve performance and endurance too.
Summary
The first indication of dysfunctional movement patterns and inadequate stabilization is often a feeling of discomfort or pain. That is, people do not develop joint and muscle pain because of what they are doing. It isn’t the activity that caused their injury. It is the inefficiency of their movements and the lack of quality of their stabilization that predisposed them to injury. Faulty movement patterns are not due to individual muscle weaknesses, but rather a lack of coordination and activation of a proper stabilization pattern. The brain, for a multitude of different reasons, has substituted the ideal stabilization pattern with one less effective. The focus of treatment and rehabilitation should be on restoring pain-free mobility and establishing efficient movement patterns with proper stabilization. We need to go beyond the myopic view that musculoskeletal conditions result from an underlying weakness. Non-weight bearing exercises that focus on training muscles in isolation while ignoring the kinetic chain will never improve someone’s functional capacity.
The most effective way of correcting a faulty stabilization pattern is to first identify exactly where in the kinetic chain or movement sequence the dysfunction appears. DNS provides an excellent method for evaluating and correcting stabilization strategies and movement patterns. DNS is based on years of observing the perfect stabilization, posture and movement of neurologically healthy infants. This serves as a gold standard of how the rest of the population should function. In addition to DNS, the use of specific chiropractic adjusting techniques and myofascial mobilization can change the quality of someone’s movement patterns and stability for life.
References:
- https://www.mlb.com/news/dizzy-dean-injured-in-1937-all-star-game/c-159226114
- Lewit K (1980) Relation of faulty respiration to posture and with clinical implications. The Journal of the American Osteopathic Association 525–529.
- Barr KP, Griggs M, Cadby T (2005) Lumbar stabilization: Core concepts and current literature, part 1. American journal of physical medicine and rehabilitation 473–480.
- Hodges PW, Richardson CA (1999) Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Archives of physical medicine and rehabilitation 1005–1012.
- Kolar P, Neurwith J, Sanda J, Suchanek V, Svata Z, et al. (2009) Analysis of diaphragm movement during tidal breathing and during its activation while breath holding using MRI synchronized with spirometry. Physiol Res 383–392.
- Kolar P, Sulc J, Kyncl M, Sanda J, Cakrt O, et al. (2012) Postural function of the diaphragm in persons with and without chronic low back pain. The Journal of orthopaedic and sports physical therapy 352–362.
About the Author:

Dr. Morris Gasparin is full body level 1 & 2 Active Release Techniques certified. He has been incorporating the DNS method of evaluation and rehabilitation since 2012 and been in private practice at Cloverdale Chiropractic since 1995.